Excerpts and Illustrations
Excerpt from “Being in the ICU room: Interacting with your loved one”
Finally, a caregiver (likely a nurse) has come to tell you that you may come to see your loved one.
He is likely surrounded by an overwhelming and confusing array of machines and monitors, with multiple tubes and wires attached to his body. Monitors might be flashing and beeping intermittently. One or more people will probably be busy in the room, moving about his bed, working at a computer, and adjusting equipment.
Do not allow yourself to be alienated or distanced from your loved one by all this equipment and activity, or by fear of being “in the way.” He is still very much the same person and has never needed you more. You belong right next to him, at the head of the bed (unless a caregiver temporarily needs to be there to do a task). You may talk to him and hold his hand, even if it is strapped down to the bed or to a board. Unless you are unusually rough or clumsy, you will not dislodge any important tubes or lines, which should be firmly taped in place. Ask the nurse if you may pull up a chair to the bedside.
Your relative is likely to be drowsy or asleep, either because of sedative medications or because of chemical or other physiological changes that occur with critical illness. If so, can he understand you, or register that you are there? No one can know for sure. In my opinion, it is best to assume that he can hear you, is aware of your presence, and can derive comfort from the sound of your voice. Talk to your relative as if he were fully conscious . . . .
Excerpt from “Being in the ICU room: Lines, tubes, wires, and machines”
Now that you have taken your rightful place by your loved one’s side, it’s time to introduce you to all the lines (small tubes or catheters), tubes, wires, and machinery. For your reference, I’ve provided an illustration of the ICU patient and room, labelled with letters corresponding to descriptions below . . . .
Excerpt from “’We need to know what your loved one would want’ - Decisions about life support and code status
Some family members are initially mystified by the question about code status. Why on earth wouldn’t you restart the heart and lungs? Isn’t that worth at least an attempt? The reason is that the very fact of needing cardiopulmonary resuscitation means that the person is very sick: in the best-case scenario, they will likely have a long and difficult hospital course; and in the worst-case scenario, they may not survive to be discharged — or they may survive but with impaired brain function and quality of life. Some patients or proxies might reasonably feel that the risks of pursuing such care are too great, particularly in cases where the patient is very elderly or terminally ill.
While a limited code status is often lumped together as “DNR/DNI,” it is important to realize that the issues for mechanical ventilation (to which “DNI” refers) and cardiac resuscitation (to which “DNR” refers) differ quite a bit . . .


Excerpt from “The breathing machine: what is a mechanical ventilator?”
Of all the machinery in your relative’s room, the mechanical ventilator (called “the ventilator” or sometimes “the vent”) is likely to loom largest – both physically and psychologically. It carries large symbolic importance – when people say that they would not want to live “on a machine,” the ventilator is what they are referring to. Yet, the ventilator generally has little effect on the course of illness, but rather is the classic example of supportive care — it is not itself a treatment. The ventilator takes some or all of the work of breathing off your relative while the lungs and the rest of the body have time to recover.
Being on a ventilator, in and of itself, has little significance in terms of “how sick” your relative is. Someone can be on a ventilator for less than a day because they require an elective surgery on their knee, for example, or because they inhaled a piece of steak and it needs to be extracted. On the other hand, severe lung disease may require prolonged ventilation — carrying a much worse prognosis (likely outcome) . . . .
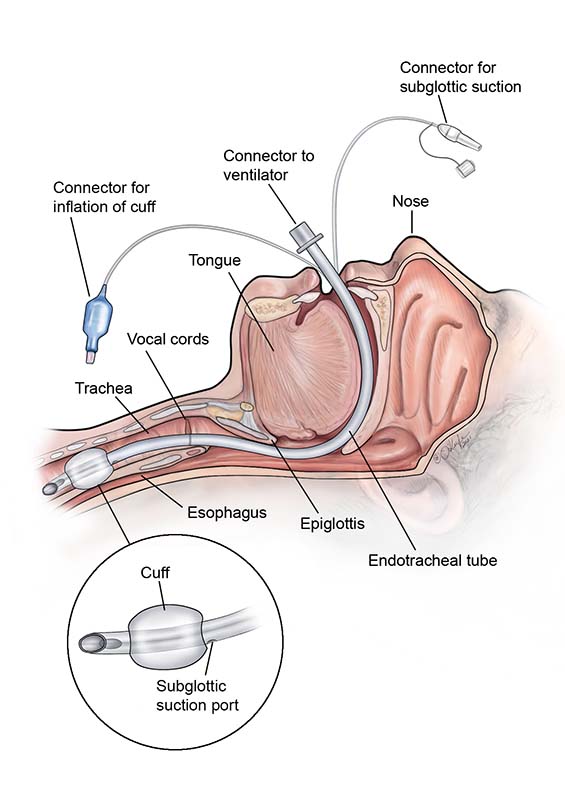
Usually, the mechanical ventilator is connected to a patient through a tube (endotracheal tube, or endotracheal tube; sometimes spoken as “E-T-tube”) that enters the mouth and terminates in the windpipe (trachea) a few inches below the vocal cords, as shown in the illustration.
Excerpt from “The breathing machine: what is a mechanical ventilator?”
The lung is like a balloon. But instead of inflating the balloon by forcing air inside, the lung is normally held in an open position — closely against the chest wall — by a vacuum seal. If air enters that tight seal, the vacuum is broken: the space between the lung and the chest wall (called the pleural space) springs open, and the lung collapses. Air in the pleural space is called a “pneumothorax.” The air can come from either inside the lung (if there is damage to the lung, for example from pneumonia), or from outside the chest wall (if there is damage to the chest, for example from a car crash or as a complication from a medical procedure like central line placement).
Alternatively, fluid can enter the pleural space, causing it to enlarge and compress the lung (as shown in the figure). Fluid in the pleural space is called a “pleural effusion.” The fluid can come from many sources – for examples, bleeding, heart failure, infection (like pneumonia), or cancer.
Excerpt from, “How could I even think about giving up?”
This question was asked of me once by a patient’s daughter, with tears in her eyes. Her mother had been in the ICU on life support for more than two weeks, and I had proposed a tracheostomy and feeding tube in anticipation of a very long course of care. The daughter was beginning to wonder whether all this was what her mother would have wanted, or even in her best interest. As her mother’s decision-maker, she was considering withdrawing life support — but she felt guilty for even considering giving up the fight. After all, wasn’t her mother engaged in the fight of her life? Didn’t she need her daughter to fight with her? This young woman was unusually courageous in asking the question aloud, but I think many people with loved ones on prolonged life support have just the same question very much in mind.
It is important to know that decisions about withdrawing life support are not monstrous – to the contrary, they are a common and necessary result of just how terribly good the ICU has become at keeping people alive. With machines to take over the work of the lungs, heart, and kidneys, and with medications to control blood pressure and fluid and electrolyte balance, we can now keep almost anyone technically “alive” — way past the point that it makes sense, in that they could return to reasonable quality of life. No one wants that for their loved one. When people die in the ICU, it is usually not because they die despite the machines and medications. Sixty-five percent of the deaths that occur in the ICU occur after a decision to withdraw care. We must recognize that family members are frequently obliged to help make decisions about when “enough is enough.”
We all die eventually. At some point, the most important question becomes not whether we will die, but how. When the time is right, shifting to the latter question is the most courageous and loving thing you can do for the patient . . .